Chronic obstructive pulmonary disease (COPD) causes factors and symptoms.
whai is chronic obstructive pulmonary disease (COPD), causes, factors and symptoms.
COPD
Chronic obstructive pulmonary disease (COPD) is a state characterized by airflow limitation owing to chronic bronchitis or emphysema. It is progressive disease and not fully reversible. COPD is a fatal inflammatory lung disease caused by a deficiency of AAT protein. Whereas AAT protein which is secreted from the liver cures and prevents the exacerbation of COPD in the lungs. AAT production is inhibited by various factors.
Formation types of Chronic obstructive pulmonary disease ( COPD)??
There are two types
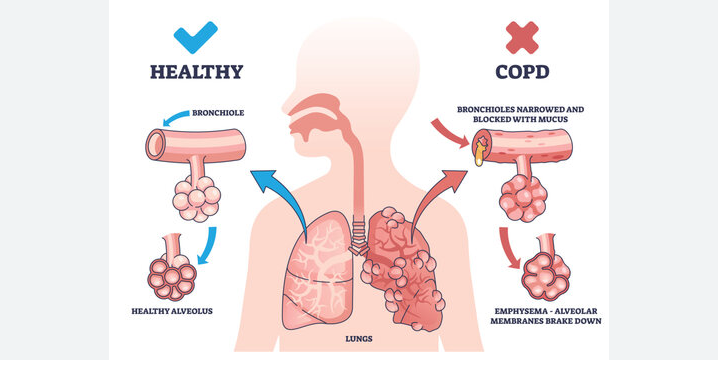
- Chronic bronchitis: It is characterized by excessive mucus production by the tracheobronchial tree. That may airway obstruction as a result of edema and bronchial inflammation. Chronic obstructive pulmonary disease (COPD) patient has a cough producing more than 30 ml of sputum in 24 hours for at least 3 months of the year for 2 consecutive years.
- Emphysema: It is characterized by permanent alveolar enlargement distal to the terminal bronchioles and destructive changes of the alveolar walls. Alveolar surface area losses and causes airway limitation.
Note: Comorbidities such as CHF, CAD, Stroke, DM, and Depression are common in COPD patients.
Causes
- Cigarette smoking
- α 1- antitrypsin ( AAT) deficiency.
- Expose to irritants such as sulfur dioxide, polluted partials, noxious gas, organic or inorganic dust or combustible fuels in the home etc.
- A history of respiratory infection or bronchial hyper reactivity.
- Social, economic or hereditary factors.
Pathophysiology
-
Chronic bronchitis
- When respiratory tissue inflamed result in vasodilation, congestion, mucosal edema, and goblet cell hypertrophy. That triggers to produce excessive amount of mucus.
- Tissue structure become changes like increase smooth muscle, cartilage atrophy, infiltration of neutrophils and other cell and impairment of cilia.
- Airway become blocked by thick, tenacious mucus secretion which trigger a productive cough.
- Alveoli become infection by various bacteria or virus like streptococcus pneumonia, Haemophilus influenza, Moraxella cattarrhalts, Staphylococcus aureus and Pseudomonas aeruginosa species. Recurrent lung infection reduce ciliary and phagocytic activity, increase mucus accumulation, weaken body’s defense and destroy further small bronchioles.
- Overall impaired gas exchange decrease blood PaO2 increase PaCO2 may result exertional dyspnea and hypercapnia.
2. Emphysema
- From the bronchitis breakdown of the bronchioles, alveolar walls and connective tissue finally resulted alveoli merge, the number of alveoli diminishes and reduce the alveolar elasticity which entrapped air.
- Finally increase lung volume decrease blood PaO2 increase PaCO2 causes exertional dyspnea and hypercapnia.
Clinical evaluation
-
Chronic bronchitis :
- Symptoms are onset after the age of 45 years.
- Productive cough in winter then progresses to years round.
- Exertional dyspnea.
- Obesity, rhonchi, wheezes and prolonged expiration.
- Right ventricular failure, peripheral edema, hepatomegaly, and cardiomegaly.
2. Emphysema
- Symptoms are onset after the age of 55 years.
- Exertional dyspnea. It may be progressive, severe, constant than Chronic bronchitis
- Weight loss
- Tachypnea
- Pursed-lips-breathing
- Prolonged expiration
- Diaphragmatic excursion
- Diminished breath sound

Diagnostic
Normally COPD common finding
- Cough
- Dyspnea
- Sputum production
- FEV1/FVC < 70%
Chronic bronchitis diagnostic
Physical finding
- Dyspnea
- Coughing, thick purulent or mucopurulent sputum that may yellow color, white, green or gray in color.
Blood test
- Polycythemia
- WBC count may increase due to infection.
- Arterial blood gas studies
!. Decrease PaO2 level ( 45 to 60 mm Hg) !!. Increase PaCO2 level ( 50 to 60 mm Hg) 4. Hypercapnia
Spirometer test
- FEV1/FVC < .08
- Increase residual lung volume
- Decrease vital capacity (VC)
- Decrease FEV1
Chest Radiograph (X-Ray)
- Lung hyperinflation
- A barrel chest
- Increase bronchovascular marking
Heart function test
- Right ventricular hypertrophy
- Tachycardia
Emphysema diagnostic
Physical finding
- Dyspnea
- Scanty sputum that is clear or mucoid.
Blood test
- Polycythemia
- WBC count may increase due to infection but infection is less common.
- Arterial blood gas studies
!. Decrease PaO2 level ( 65 to 75 mm Hg) or may not change. !!. Increase PaCO2 level ( 50 to 60 mm Hg) 4. Hypercapnia
Spirometer test
- FEV1/FVC < .08
- Increase residual lung volume and TLC
- Decrease vital capacity (VC)
- Decrease FEV1
Chest Radiograph (X-Ray)
- Lung hyperinflation
- Flattened diaphragm
- Vertical heart
- Enlarged anteroposterior chest diameter
- Decreased vascular marking
Heart function test
- Right ventricular hypertrophy
- Tachycardia
Note: patient with potentially fatal COPD should be quickly identify and aggressively managed Need to hospitalization.
Prevention and treatment of chronic obstructive pulmonary disease ( COPD).
Exercise-induced bronchospasm (EIB )
You can prevent exacerbation Due to exercise By using medication .
1.1, Short acting beta agonist ( eg. Albuterol) Should be administered 15 minutes before exercise.
1.2, long acting beta agonist and formoterol should be administered 30 to 60 mins before exercise.
Concurrent disease
Allergic rhinitis sinusitis and Gastroesophageal Reflux disease (GERD), vocal cord dysfunction and obstructive sleep apnea frequently coexist with asthma. It should be better to management of this concurrent disease by medication with chronic obstructive pulmonary disease treatment.
2.1. For Gastroesophageal Reflux disease Medication should be use such as PPI (eg. esomeprazol, Pantoprazol) or H2 receptor antagonist (eg, Famotidin)
2.2. For allergic rhinitis medication should be used such as antihistamine ( eg. rupatidin. cetirizine)
There are more different factors which may affect chronic obstructive pulmonary disease condition. To prevent COPD we should know well about chronic obstructive pulmonary disease causes and symptoms.
If anyone want to more information please send to me your question through the given email address.
Email address: mallicktarun@rocketmail.com
For getting treatment base suggestion please contact or request an appointment.
You may also visit you tube video channel that may helpful to you.